Mestinon
By F. Ben. Augustana College, Sioux Falls South Dakota.
At optimum temperatures of 20–25 C with sufficient moisture and oxygen buy generic mestinon 60mg on-line spasms with stretching, an infective larva in the egg develops within about three to six weeks. Human infections result from peroral ingestion of eggs containing larvae, which hatch in the upper small intestine and penetrate into the veins of the intestinal wall. Via tracheopharyngeal migration they finally reach the digestive tract, where they further differentiate into adults in the small intestine. Female from the small intestine; first-stage larva (L1) shed in stool; L2 larva; infective L3 larva; development of L1 larva to adult stages including four moltings (); free-living male (not host-bound); free- living female; egg of free-living generation; larva hatched from egg, develops into infective larva including two moltings. Duration of life cycle about three weeks, lifespan on host usually four to five weeks, rarely as long as two months; can survive without a host at 10–20C for about one week and at 0–10C for approximately 10 days. Bite reactions on the body, espe- cially around the underwear, are indicative of body louse infestation. Serology; worm eggs in stool (larvae) Serology (larvae) Serology (specific IgE) (worm eggs in stool) spp. Empyema Microscopy and culture from pleural pus specimen Numerous other bacteria are potential pathogens Pulmonary abscess Usually endogenous Microscopy and culture from Necrotizing pneumonia infections with Gram- transtracheal or bronchial negative/Gram-positive aspirate, bronchoalveolar mixed anaerobic flora lavage or lung biopsy. Urogenital Tract Urethrocystitis Microscopy and culture; test Pyelonephritis Other midstream urine for significant bacteriuria (p. Bacteriuria (5–10%) often <104/ml – Unknown pathogens (20%) Microsporosis of the spp. Usage subject to terms and conditions of license Spirurida Tapeworms Tapeworms Tuberculosis Tuberculosis Whooping cough (pertussis) Whooping cough (pertussis) . He has also taught at the New School for Social Research, Michigan State University, and at the University of Tübingen in Germany. Stangor is the recipient of research grants from the National Institute of Mental Health and from the National Science Foundation. He has published seven books and over 70 research articles and book chapters and has served as an associate editor of the European Journal of Social Psychology. He has served as the chair of the executive committee and is currently executive officer for the Society for Experimental Social Psychology. Stangor‘s research interests concern the development of stereotypes and prejudice and their influences upon individuals who are potential victims of discrimination. Stangor regularly teaches Social Psychology, Research Methods, and at the graduate level, Fundamentals of Social Psychology and Group Processes. Stangor is chair of the undergraduate committee in the psychology department and has won the distinguished teaching award from the University of Maryland. One important resource was an advisory board of instructors from across the country. Their thoughtful and insightful feedback throughout development was invaluable in creating this first edition. Isaak, University of Louisiana at Lafayette Kerry Jordan, Utah State University Jerwen Jou, University of Texas–Pan American Peggy Norwood, Community College of Aurora Karen Rhines, Northampton Community College Eva Szeli, Arizona State University Anton Villado, Rice University Introduction to Psychology also benefited from reviews at various stages of the book‘s development. Achorn, The University of Texas at San Antonio Mara Aruguete, Lincoln University David Carlston, Midwestern State University Jenel T. Fernando, California State University, Los Angeles William Goggin, University of Southern Mississippi Karla A. Lassonde, Minnesota State University, Mankato Greg Loviscky, Pennsylvania State University Michael A. Peteet, University of Cincinnati Brad Pinter, Pennsylvania State University, Altoona Steven V. Isaak, University of Louisiana at Lafayette, for his work on the accompanying Test Item File and PowerPoint slides; and to Chrissy Chimi and Stacy Claxton of Scribe, Inc. Completion of the book and supplements required the attention of many people, including Michael Boezi, who signed the book and supported my efforts from beginning to end; Pam Hersperger, who managed the book through development; and Gina Huck Siegert, who worked closely with me on all aspects of the project. I was able to give a lecture on the sympathetic nervous system, a lecture on Piaget, and a lecture on social cognition, but how could I link these topics together for the student? I felt a bit like I was presenting a laundry list of research findings rather than an integrated set of principles and knowledge.
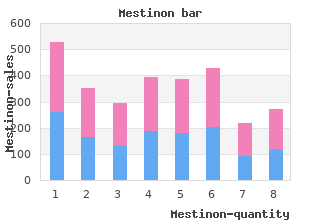
Stunkard (1984) suggested that obesity should be categorized as either mild (20–40 per cent overweight) buy discount mestinon 60mg on-line muscle relaxant alcohol addiction, moderate (41–100 per cent overweight) or severe (100 per cent overweight) obesity. However, it does not allow for differences in weight between muscle and fat – a bodybuilder would be defined as obese. Overall, people in Northern and Western Europe are thinner than Eastern and Southern Europe and women are more likely to be obese than men. Physical problems Obesity has been associated with cardiovascular disease, diabetes, joint trauma, back pain, cancer, hypertension and mortality (e. The effects of obesity are related to where the excess weight is carried; weight stored in the upper body, particularly in the abdomen, is more detrimental to health than weight carried on the lower body. It is interesting to note that although men are more likely than women to store fat on their upper bodies, and are therefore more at risk if obese, women are more concerned about weight than men and most treatment studies examine women. It has been suggested that most problems seem to be associated with severe obesity and weights in the top 10 per cent (Wooley and Wooley 1984). Psychological problems Research has examined the relationship between psychological problems and obesity. The contemporary cultural obsession with thinness, the aversion to fat found in both adults and children and the attribution of blame to the obese may promote low self- esteem and poor self-image in those individuals who do not conform to the stereo- typically attractive thin image. Furthermore, Hopkinson and Bland (1982) reported that one-fifth of their sample of obese subjects, also waiting for surgical treatment, reported having at least one period of clinical depression requiring treatment. However, it is possible that depressed obese individuals are more likely to seek treatment for their obesity than those who are not depressed and that there may be many obese individuals who are quite happy and therefore do not come into contact with health professionals. Therefore, although some obese people may be depressed there is no consistent support for a simple relationship between body size and psychological problems. The theories relating to the causes of obesity include both physiological theories and behavioural theories. Physiological theories Several physiological theories describe the possible causes of obesity. Genetic theories Size appears to run in families and the probability that a child will be overweight is related to the parents’ weight. For example, having one obese parent results in a 40 per cent chance of producing an obese child and having two obese parents results in an 80 per cent chance. In contrast, the probability that thin parents will produce overweight children is very small, about 7 per cent (Garn et al. However, parents and children share both environment and genetic constitution, so this likeness could be due to either factor. Twin studies Twin studies have examined the weight of identical twins reared apart, who have identical genes but different environments. Studies have also examined the weights of non-identical twins reared together, who have different genes but similar environments. The results show that the identical twins reared apart are more similar in weight than non-identical twins reared together. However, the role of genetics appears to be greater in lighter twin pairs than in heavier pairs. Such studies compare the adoptees’ weight with both their adoptive parents and their biological parents. The results showed a strong relationship between the weight class of the adoptee (thin, median weight, overweight, obese) and their biological parents’ weight class but no relationship with their adoptee parents’ weight class. This relationship suggests a major role for genetics and was also found across the whole range of body weight. Interestingly, the relationship to biological mother’s weight was greater than the relationship with the biological father’s weight. Research also suggests that the primary distribution of this weight (upper versus lower body) is also inherited (Bouchard et al. Metabolic rate, the number of fat cells and appetite regulation may be three factors influenced by genetics. Metabolic rate theory The body uses energy for exercise and physical activity and to carry out all the chemical and biological processes that are essential to being alive (e. The rate of this energy use is called the ‘resting metabolic rate’, which has been found to be highly heritable (Bouchard et al.
He has smoked 10–15 cigarettes per day for 25 years and drinks around 30 units of alco- hol each week mestinon 60 mg low cost muscle relaxant non sedating. He has been feeling more tired recently and had put this down to pressure of work. Examination There is mild tenderness in the epigastrium, but no other abnormalities. The high red cell count with low haemoglobin shows that the haemoglobin content of the cells is reduced. The blood film confirms that the cells are microcytic and low in haemoglobin (hypochromasia). The commonest cause of iron-deficiency anaemia in a man is gastrointestinal blood loss. The abdominal pains would be consistent with those from a peptic ulcer, especially a duodenal ulcer when there is more often some relief from food. The diagnosis should be established by endoscopy because alternative diagnoses such as carcinoma of the stomach cannot be ruled out from the history. In this case, an endoscopy confirmed an active duodenal ulcer and samples were positive for Helicobacter pylori. He was given strong recommendations to stop smoking and to address his excessive alcohol consumption. The iron deficiency was corrected by additional oral iron which was continued for 3 months to replenish the iron stores in the bone marrow. Repeat endoscopy to show healing con- firms the original diagnosis of benign ulceration. She struggles to get out of bed by herself and she has difficulty lifting her hand to comb her hair. She has lost 4 kg in weight, and has noticed some sweats which seem to occur at night. Patients may pres- ent primarily with polymyalgia-type symptoms (proximal muscle pain and stiffness most marked in the mornings) or temporal arteritis symptoms (severe headaches with tenderness over the arteries involved). Patients may have systemic symptoms such as general malaise, weight loss and night sweats. In polymyalgia, the main symptoms are muscle stiffness and pain which may simulate muscle weakness. When there are headaches and giant cell arteritis is suspected, a temporal artery biopsy should be performed. However, the histology may be normal because the vessel involve- ment with inflammation is patchy. Nevertheless, a positive result provides reassurance about the diagnosis and the need for long-term steroids. This patient has clear evidence of giant cell arteritis (also known as temporal arteritis although other vessels are involved), and is at risk of irreversible visual loss either due to ischaemic damage to the ciliary arteries causing optic neuritis, or central retinal artery occlusion. The patient should immediately be started on high-dose prednisolone (before the biopsy result is available). She was sitting down with her husband when the weak- ness came on and her husband noticed that she slurred her speech. Her husband has noticed two to three episodes of slurred speech last- ing a few minutes over the last 6 months but had thought nothing of it. Two months earlier she had a sensation of darkness coming down over her left eye and lasting for a few minutes. Her dorsalis pedis pulses are not palpable bilaterally and her posterior tibial is weak on the left and absent on the right. She is at increased risk of cerebrovascular disease because of her smoking, hypertension and dia- betes. Two months before her admission she had an episode of amaurosis fugax (transient uniocular blindness) which is often described as like a shutter coming down over the visual field of one eye.
Edward recovers cheap mestinon 60 mg fast delivery spasms 1983 trailer, but may be left with some long-term neurological complications (e. Chapter 4 Artificial ventilation Fundamental knowledge Respiratory physiology Normal (negative pressure) breathing Dead space Normal lung volumes Experience of nursing ventilated patients Introduction Intensive care units developed from respiratory units: the provision of mechanical ventilation, and thus the care of ventilated patients, is fundamental to intensive care nursing. Nurses should have a safe working knowledge of whichever ventilators they use— manufacturers’ literature and company representatives are usually the best source for this. This chapter discusses the main components of ventilation (tidal volume, I:E ratio) and the more commonly used modes. The chapter ends by identifying the complication of positive pressure ventilation on other body systems. Artificial ventilation should meet physiological deficits (metabolic oxygen demand and carbon dioxide elimination). These terms are therefore not used here, but readers should be aware of their existence and meanings. Carbon dioxide removal requires active tidal ventilation and so is affected by inspiratory pressure tidal volumes expiratory time. Manipulating these factors can optimise ventilation while minimising complications. Normal adult alveolar ventilation is about four litres each minute; normal cardiac output is about five litres each minute. Shunting can also occur at tissue level (reduced oxygen extraction ratio, see Chapter 20). Care of ventilated patient The care of ventilated patients should be holistic—the sum of many chapters in this book, especially in Part I. Artificial ventilation causes potential problems with: ■ safety ■ replacing normal functions ■ system complications Ventilated patients have respiratory failure, so ventilator failure or disconnection may be fatal. Modern ventilators include alarms and default settings, but each nurse should check, and where appropriate reset, alarm limits for each patient; Pierce (1995) recommends a ‘rule of thumb’ margin of 10 per cent for alarm settings. Alarms may fail and so nurses should observe ventilated patients both aurally and visually. This necessitates appropriate layout of bed areas to minimise the need for nurses to turn their backs on their patients. Back-up facilities in case of ventilator, power or gas failure should include: ■ manual rebreathing bag, with suitable connections ■ oxygen cylinders ■ equipment for reintubation Additional safety equipment may also be needed (e. Positive pressure ventilation is unphysiological; increased intrathoracic pressure compromises many other body systems (especially cardiovascular), causing problems identified later in this and many other chapters. Intensive care nursing 28 Fighting ventilation (dysynchrony between ventilator and patient-initiated breaths) should not occur, almost all modern ventilators incorporate trigger modes. However patient discomfort from ventilation (coughing, gagging—often from oral tracheal tubes, including biting on tubes) may cause problems. Nurses should monitor effects of ventilation, providing comfort where possible (e. When physical restraint cannot be avoided, it is best limited to manual restraint, using the minimum force necessary, which should be released as soon as possible. Tidal volume Tidal volume affects gas exchange, but can also cause shearing damage to lungs; settings should therefore balance immediate needs of oxygenation and carbon dioxide removal against potential lung damage/healing. While not too dissimilar to peak flow volumes, normal respiration preferentially distributes air to dependent lung bases (especially when standing) (Ryan 1998), matching maximal ventilation with optimum perfusion; lying down reduces the functional residual capacity by about one-third, thus artificial ventilation distributes gas unevenly, overdistending upper lung zones (Ryan 1998). Patients at greatest risk from alveolar trauma usually have poor compliance, low functional lung volumes and hypoxia, creating dilemmas between adequate oxygenation and risks of lung damage. When patient-initiated negative pressure exceeds the set trigger level, patients can ‘breath through’ the ventilator. With most ventilatory modes, triggered breaths are in addition to preset volumes, but included in measured expired minute volume. Incorporating triggering/sensitivity into ventilators aids weaning and facilitates patient comfort by overcoming the problems of ‘fighting’. At rest, self-ventilation negative pressure is approximately −3 mmHg (Adam &; Osborne 1997); trigger levels below this can cause discomfort (fighting). Early methods of immersing expiratory port tubing into water (hence measurement in cmH2O) have been replaced by resistance valves (usually incorporated into ventilators). However, frequent small tidal volumes may achieve minute volume limits without clearing airway dead space. Once a breath is triggered, pressure support delivers gas until the preset peak airway pressure is reached.
Outcome measures in- that cheap 60 mg mestinon with mastercard back spasms 5 weeks pregnant, at the very least, open-ended interviews in- cluded self-esteem (Rosenberg, 1965); overall emo- volved aspects of knowing, being with, and main- tional disturbance, anger, depression, anxiety, and taining belief. We suspected that if doing-for and confusion (McNair, Lorr, & Droppleman, 1981); enabling interventions specifically focused on com- and overall miscarriage impact, personal signifi- mon human responses to health conditions were cance, devastating event, lost baby, and feeling added, it would be possible to transform the tech- of isolation (investigator-developed Impact of niques of phenomenological data gathering into a Miscarriage Scale). That conversation ultimately A more detailed report of these findings is pub- led to my design of a caring-based counseling lished elsewhere (Swanson, 1999a). The next thing I knew, I was writing a proposal Participants were within five weeks of loss at en- for a Solomon four-group randomized experimen- rollment; 89 percent were partnered, 77 percent tal design (Swanson, 1999a, 1999b). The primary purpose of the study tional disturbance, anger, and depression; and (2) was to examine the effects of three one-hour-long, with the passage of time, women attributed less caring-based counseling sessions on the integration personal significance to miscarrying and realized of loss (miscarriage impact) and women’s emo- increased self-esteem and decreased anxiety, de- tional well-being (moods and self-esteem) in the pression, anger, and confusion. Additional aims of the In summary, the Miscarriage Caring Project study were to (1) examine the effects of early versus provided evidence that, although time had a heal- delayed measurement and the passage of time on ing effect on women after miscarrying, caring did women’s healing in the first year after loss, and (2) make a difference in the amount of anger, depres- develop strategies to monitor caring as the inter- sion, and overall disturbed moods that women ex- vention/process variable. This study was unique An assumption of the caring theory was that in that it employed a clinical research model to the recipient’s well-being should be enhanced by determine whether or not caring made a difference. Swanson: A Program of Research on Caring 357 I believe that its greatest strength lies in the fact that presession moods (thus enabling examination of the intervention was based both on an empirically the association between counselor presession derived understanding of what it is like to miscarry mood and self or client postsession ratings of and on a conscientious attempt to enact caring in caring). Of course, to complete the Caring Professional Scale (investi- the greatest limitation of that study is that I derived gator-developed). Women, having been left alone the caring theory (developed from the interven- to complete the measure, were asked to place the tion) and conducted most of the counseling ses- evaluations in a sealed envelope. Hence, it is unknown whether similar results in another room, the counselor wrote out her would be derived under different circumstances. I am currently making consisted of 18 items on a five-point Likert-type a concerted effort to rectify this situation and to ex- scale. It was developed through the Miscarriage amine what it is like for diverse groups of women to Caring Project and was completed by participants experience both miscarriage and caring. The items document that, as claimed, caring had indeed oc- included: “Was the health-care provider that just curred. First, approximately 10 percent of the inter- took care of you understanding, informative, aware vention sessions were transcribed. The items were derived from the car- study, found she could not approach analysis of the ing theory. Three negatively worded items (abrupt, transcripts naively—that is, with no preconceived emotionally distant, and insulting) were dropped notions, as would be expected in the conduct of due to minimal variability across all of the data sets. Hence, she employed For the counselors at one, five, and eleven weeks both deductive and inductive content analytic tech- postloss, Chronbach alphas were. The lower reliability estimates question, “Is there evidence of caring as defined by were because the counselors’ caring professional Swanson [1991] on the part of the nurse coun- scores were consistently high and lacked variability selors? Phrases were Noteworthy findings include the following: coded for which (if any) of the five caring processes were represented by the emic utterances. Each counselor had a full range of presession counselor statement was then further coded for feelings, and those feelings/moods were, as which subcategory of the five processes was repre- might be expected, highly intercorrelated. The caring professional scores were extremely ance of the nurse counselor could be accounted for high for both counselors, indicating that, over- by one of the subcategories. One of the counselors was a psychiatric nurse by completed a Profile of Mood States (McNair, Lorr, background. In the first part, a meta-analysis of 18 quan- case, depression and confusion) were signifi- titative studies of caring actions was performed. During Session I, women discussed in-depth provided; (2) knows how to give shots and manage what the actual events of miscarrying felt like. By contrast, the that her own vulnerabilities were a bit less top five caring behaviors valued by nurses were: (1) veiled. The second go out in public as a woman who had miscar- part of the caring actions summary was a review of ried), was the only session in which the other 67 interpretive studies of how caring is expressed counselor’s vulnerabilities came through. These counselor, having just gone through a divorce, qualitative studies were classified under Swanson’s was probably least able to hide her presession caring processes, thus lending credibility to caring moods (depression, (p. In summary, this literary notably, there was an association between this meta-analysis clarified what “caring” means, as the counselor’s presession tension and the client’s term is used in nursing, and validated the general- caring professional rating (p. Analysis of Caring Couples Miscarriage Another recent project was an in-depth review of the literature. This literary meta-analysis is pub- Healing Project lished elsewhere (Swanson, 1999). Proposed were five make a difference in men and women’s healing after domains (or levels) of knowledge about caring in miscarriage.
Paramedics bring in a 54-year-old man who was found down in his apartment by his wife buy cheap mestinon 60mg on-line spasms above ear. Records indicate that he has a past medical history of hyper- tension, diabetes, dementia, and benign prostatic hypertrophy. His lungs are clear to auscultation, with scant crack- les at the bases, and his abdomen is soft, nontender, and nondistended. The nurse places the patient on a cardiac monitor and begins to get his vital signs. While the nurse is obtaining the vital signs, he notices the patient suddenly becomes unresponsive. A 34-year-old woman with no known medical problems is having a sushi dinner with her husband. Halfway through dinner, she begins scratching her arms and her husband notices that her face is flushed. The itching intensifies and she begins to feel chest pain, shortness of breath, and dizziness. As you perform laryngoscopy to intubate the patient, you easily visualize the vocal cords and subsequently pass the orotracheal tube through the vocal cords. You place the colorimetric end-tidal carbon diox- ide device over the tube and get appropriate color change. There are equal, bilateral breath sounds on auscultation and you observe chest wall motion with ventilation. He has a past medical history of hypertension and diabetes and both are well controlled on hydrochlorothiazide, benazepril, atenolol, and metformin. He has grossly normal peripheral sensation, but no motor strength in all four extremities. He has been unable to get out of bed for the past day because of dizziness when changing position. A few minutes later, the nurse alerts you that the patient has become unconscious. A 48-year-old man with a medical history of cirrhosis caused by hepatitis C has been vomiting bright red blood for 1 day. You are concerned about meningo- coccemia and immediately start ceftriaxone and vancomycin. His medications include albuterol, ipratropium, prednisone, hydrochlorothiazide, and atenolol. A 64-year-old woman with a history of depression and hypertension was found down by her husband and brought in by the paramedics. Her husband says that she has recently been depressed and expressed thoughts of suicide. On arrival, the patient is obtunded, but responds to pain and is maintaining her airway. A 19-year-old man suffers a single gunshot wound to the left chest and is brought in by his friends. Chest radiograph shows a globular cardiac silhouette, but a normal mediastinum and no pneumothorax. As your colleague is performing a physical examination, you place the portable ultrasound on the heart and see a thin echo-free area around the heart with right atrium and right ventricular collapse. You administer aspirin, nitroglycerin, and morphine sulfate and wait for his laboratory results. Her caretaker reports that she is having mid-epigastric pain and had one episode of nonbloody, nonbilious vomiting prior to arrival. On examination, the abdomen is soft, nontender, with no masses, rebound or guarding. You send her blood to the laboratory and order a radiograph of her chest that is shown below. Support for this diagnosis includes an older patient with a history of coronary artery disease, and new mental status changes cou- pled with signs of volume overload. Hypovolemic shock (a) occurs when there is inadequate volume in the circulatory system, resulting in poor oxygen delivery to the tissues. Neuro- genic shock (b) occurs after an acute spinal cord injury, which disrupts sympathetic innervation resulting in hypotension and bradycardia.
Although the prescriber specifies a route in the medication order purchase mestinon 60mg with mastercard back spasms 36 weeks pregnant, the patient’s current condi- tion might indicate a different route is appropriate. If the route is no longer appropriate, then the nurse should con- tact the prescriber and obtain an order to use an alternate route that is appro- priate for the patient’s condition. Sometimes the dose doesn’t match the prepared dose that the nurse has on hand requiring the nurse to calculate the dose. For example, the prescriber might write a med- ication order for 800 mg of ibuprofen. The nurse might have on hand 200 mg tablets and will have to calculate that the patient must be administered 4 tablets of 200 mg of ibuprofen. With some drugs the prescriber will order a dose based on the weight of the patient. It is the nurse’s responsibility to calculate the actual dose after weighing the patient. The nurse has 200 mg/5 mL on hand and calculates that the correct dose for the patient is 20 mL. The patient might have developed a condition since being assessed by the prescriber that makes it inappropriate to receive the medication. The nurse must review the drug’s profile in the drug manual to determine the drug’s con- traindications and then determine if they apply to the patient. If so, then the nurse must contact the prescriber to advise of the patient’s condition. This is particularly important since different healthcare professionals might prescribe the patient drugs. For example, the patient might be scheduled for an angiogram in 24 hours and the prescriber has a standing medication order for Glucophage. Gluco- phage reacts with contrast dyes and therefore cannot be administered to the patient within 24 hours of any dye procedures such as an angiogram. However, withholding medications should only be done after the healthcare provider has been notified. Drugs can have known side effects—some of which the patient can toler- ate and others that result in an adverse reaction. The nurse must review the pro- file of the drug in the drug manual to determine any side effects and adverse reactions that it might cause and monitor the patient for such signs and symp- toms. The nurse should alert the patient to the possible side effects before admin- istering the medication. In addition, the nurse can prepare to deal with a possible adverse reaction the patient might have to a medication. For example, some opioids such as morphine sulfate can cause respiratory depression. Assessment Required for Specific Drugs Besides contraindications for a drug, the drug’s profile in the drug manual also provides the nurse with the pharmacologic response of the drug (see Chapter 2)— how the drug works in the body. Knowing this, the nurse can assess the patient to determine if the patient’s body will be able to metabolize and eliminate the medication. Here are the areas that the nurse needs to consider: • Absorption The patient must be able to absorb the medication. In order for this to occur, some drugs must bind to protein, which carries drug particles through the veins and arteries. If the patient has low protein levels, some drug particles are unable to bind to the protein and the unbound drug par- ticles are free drug which can possibly result in a toxic effect. If the patient has a low albumin level, there will be less Dilantin bound to protein. The patient will be receiving the proper therapeutic dose but because much of it is not bound to protein, the serum levels of free drug will be too high—causing toxicity. If the patient’s liver isn’t functioning properly, then the drug particles are not metabo- lized and cannot be excreted from the body. This results in a buildup of the drug and can possibly cause toxicity in the patient. It is important to remember that inadequate liver function is not always caused by liver disease.