Imitrex
By T. Aidan. Linfield College.
The goal of these organizations is to produce reports to help shape sound policies cheap 25 mg imitrex spasms just before falling asleep, inform public opinion, and advance the pursuit of science, engineering, and medicine. Other vitamin studies report evidence eating adequate amounts of fresh fruits and vegetables. In the Physicians’ Health Study, 22,071 examination, including appropriate laboratory testing, do American male physicians (age 40 to 84 years, 11% smok- not have any documentable complications of the disease, ers and 39% former smokers) were randomly assigned to are at very high risk for eventually developing them. This receive β-carotene (50 mg) or aspirin compared to pla- tenet is central to a preventive medicine approach to meta- cebo. Hypovitaminosis als lose excess fat mass, and traditionally this has been the D with secondary hyperparathyroidism has been reported goal of treatment. What Nutritional Recommendations are Adult feeding behavior is rooted from childhood expe- Appropriate for Weight Management? Therefore, it is important to consider the role that adults play in rearing children, since a number of factors Eat little, sleep sound. Both household food availability (foods English Proverb present in the house) and accessibility (whether available food is in a form or location that facilitates their consump- 4. Home availability and taste preferences are the stron- lipidemia, and hyperglycemia. Parental feeding style may also have a Clinical Practice Guidelines for Healthy Eating, Endocr Pract. On the other hand, consump- the majority of offerings are high in fats and concentrated tion of low-energy-dense foods (i. Nutrition should also be a part of the cur- Additional behaviors associated with obesity in adults riculum to enhance student’s skills for adopting a healthier include night eating, snacking, and alcohol consumption. Each of these behaviors may to healthy eating patterns among neighborhood residents. Low-income and minor- tunity to promote healthy eating in children, adolescents, ity neighborhoods have fewer chain supermarkets than and adults. In general, population groups that suffer the worst 28 Clinical Practice Guidelines for Healthy Eating, Endocr Pract. Thus, retail lent in foods, likely owing to the availability of inexpen- food environments at both the community level (presence sive corn and soybeans. In the American food supply, per of supermarkets) and the consumer level (healthful, afford- capita daily supply of added fats and oils increased 38% able foods in food stores) are promising venues for positive from 1970 to 2000. Low-income ity, and food safety) are of crucial importance in shaping families spend less on fruits and vegetables than do higher and maintaining nutrition and eating habits. This is because the cur- of eating behavior include the social, physical, and mac- rent structure of food prices is that high-sugar and high-fat rolevel environments we live in. Thus, low-income includes interactions with family, friends, peers, and others families may select energy-dense (albeit low-cost) foods as in the community and may impact food choices through a way to save money. Many of these factors require transcultural- current obesogenic environment warranting public health ization in order to optimize implementation for individuals intervention. The challenge then is to shift the Understanding common religious and ethnic food prac- advertising and marketing emphasis to healthier child- and tices is important in nutritional planning and education. Ads should be devel- Examples of this include: oped with practical nutrition messages that are scientif- • prohibition of pork for Muslims, Jews, and cally precise yet also acknowledge the essential factors that Seventh Day Adventists drive feeding behaviors. With the advent of computers and video terns, rituals, and celebrations, and games, “screen time” has increased in American society. Culturally appropriate nutrition counseling and Microenvironment—Physiology and awareness of religious practices are important for Molecular Defnition improving health issues such as obesity. The control of eating behavior is not restricted to cog- nitive, behavioral, and environmental factors. United are peripheral sensors (gut, adipose tissue, liver, and skel- States farm policy for commodity crops has made sugar etal muscle) that provide signals to the brain about the fed and fat some of the most inexpensive foods to produce. The brain translates this feedback Clinical Practice Guidelines for Healthy Eating, Endocr Pract. Behavioral modifcation refers to a set of prin- ety, food seeking, and other behaviors.
Nursing staff who administer ‘off-label’ medications also have a duty of care to the patient cheap 25 mg imitrex mastercard spasms rectal area. Two or more Drugs When two or more drugs are mixed in a syringe the diluent is usually water for injection. If compatibility/stability data is available for an alternative diluent then that diluent should be used 18 8. Morphine: Drug combinations for subcutaneous infusion that are stable for 24 hours • These are not clinical doses to prescribe. Use the minimum effective dose and titrate according to response • Monitor closely for visible signs of incompatibility such as the solution becoming cloudy, changing colour or the appearance of crystals Drug Combination Maximum concentrations of two drug combinations that are physically stable 17ml in 20ml syringe 22ml in 30ml syringe Morphine Sulphate 300mg Cyclizine 150mg Morphine Sulphate 300mg Glycopyrronium bromide 1200micrograms Morphine Sulphate 400mg Haloperidol 10mg Morphine Sulphate 300mg Hyoscine butylbromide 120mg Morphine Sulphate 450mg Hyoscine hydrobromide 1200micrograms Morphine Sulphate 300mg Levomepromazine 100mg Morphine Sulphate 120mg 160mg Metoclopramide 60mg 80mg Morphine Sulphate 300mg 380mg Midazolam 30mg 40mg Morphine Sulphate 400mg 500mg Octreotide 400micrograms 500micrograms 19 Drug Combination Maximum concentrations of three drug combinations that are physically stable 17ml in 20ml syringe 22ml in 30ml syringe Morphine Sulphate 40mg Cyclizine 100mg Haloperidol 2. Diamorphine: Drug combinations for subcutaneous infusion that are stable for 24 hours • These are not clinical doses to prescribe. Use the minimum effective dose and titrate according to response • Monitor closely for visible signs of incompatibility such as the solution becoming cloudy, changing colour or the appearance of crystals Drug Combination Maximum concentrations of two drug combinations that are physically stable 17ml in 20ml syringe 22ml in 30ml syringe Diamorphine 340mg Cyclizine 150mg Diamorphine 425mg Glycopyrronium bromide 1200micrograms Diamorphine 800mg Haloperidol 10mg Diamorphine 1200mg Hyoscine butylbromide 120mg Diamorphine 1200mg Hyoscine hydrobromide 1200micrograms Diamorphine 90mg Ketorolac 30mg Diamorphine 850mg Levomepromazine 100mg Diamorphine 2550mg 3300mg Metoclopramide 85mg 110mg Diamorphine 560mg 720mg Midazolam 80mg 100mg Diamorphine 425mg Octreotide 900 micrograms 21 Drug Combination Maximum concentrations of three drug combinations that are physically stable 17ml in 20ml syringe 22ml in 30ml syringe Diamorphine 340mg Cyclizine 150mg Haloperidol 10mg Diamorphine 800mg 1000mg Haloperidol 7. Oxycodone: Drug combinations for subcutaneous infusion that are stable for 24 hours • These are not clinical doses to prescribe. Use the minimum effective dose and titrate according to response • Monitor closely for visible signs of incompatibility such as the solution becoming cloudy, changing colour or the appearance of crystals Drug Combination Maximum concentrations of two drug combinations that are physically stable 17ml in 20ml syringe 22ml in 30ml syringe Oxycodone Do not mix - Do not mix - Cyclizine Incompatible Incompatible Oxycodone 140mg Haloperidol 10mg Oxycodone 140mg 180mg Hyoscine butylbromide 40mg 50mg Oxycodone 130mg Hyoscine hydrobromide 1200micrograms Oxycodone 85mg Ketorolac 30mg Oxycodone 120mg Levomepromazine 100mg Oxycodone 80mg 100mg Metoclopramide 40mg 50mg Oxycodone 80mg 100mg Midazolam 40mg 50mg Oxycodone 80mg 100mg Octreotide 400micrograms 500micrograms 23 Drug Combination Maximum concentrations of three drug combinations that are physically stable 17ml in 20ml syringe 22ml in 30ml syringe Oxycodone 80mg 100mg Haloperidol 2. Drug Conversions Converting to Diamorphine or Morphine Diamorphine and Morphine are the opioids of choice for moderate to severe pain. Diamorphine is particularly suitable for use in a syringe pump because it is highly soluble in small volumes. To convert from oral morphine to subcutaneous diamorphine: The total 24-hour dose of oral morphine should be divided by 3. To convert from oral morphine to subcutaneous morphine: The total 24-hour dose of oral morphine should be divided by 2. Total 24 hours oral morphine dose: 120 mg + 120 mg + 40 mg + 40 mg + 40mg = 360 mg. Breakthrough analgesia Breakthrough analgesia should still be prescribed subcutaneously when a th continuous infusion is in use. If the dose is difficult to calculate, round up or down to the nearest easy dose to achieve. Caution: Breakthrough analgesia given for movement related pain or incident pain in a patient whose background pain is satisfactorily controlled should not normally be added into the regular 24hour dose as toxicity may ensue. Also inhibits IgE synthesis, attenuates mucous secretion and eicosanoid generation, up-regulates beta-receptors, promotes vasoconstriction, suppresses inflammatory cell influx, and prevents / controls inflammation. Require 4-6 weeks of around-the-clock use for full effect; often misperceived as “rescuers” for acute attacks. Other strategies: Give once daily inhalation if appropriate; rinse mouth after each administration. May also slightly affect prepubertal growth in children with long-term use, decreasing adult height by approximately 1 cm. Nevertheless, close monitoring of behavior is warranted and further reviews are ongoing. Patients should be observed for 2 hours after first 3 injections, then for 30 minutes after subsequent injections, and should be provided with and trained on how to use self-injected epinephrine. Long-term- adrenal insufficiency, growth suppression in children, osteoporosis, cataract formation, glaucoma, dermal thinning Medication (brand name) Availability Adult Dose Child Dose Notes Prednisone 1, 2. Step 3 Step 4 or 5 Recommended Step for Initiating Step 1 Step 2 Consider short course of oral systemic corticosteroids for Therapy all ages In 2-6 weeks, evaluate level of asthma control that is achieved and adjust therapy accordingly. The Treatment-related adverse level of intensity does not correlate to specific levels of control but should be considered in the effects overall risk assessment. Purpose This Guideline provides recommendations regarding best practice for avoidance of issues related to animal products, whether for patient safety or cultural reasons. Guideline for the use of medicines/pharmaceuticals of animal origin Guidance Statement People who are allergic to certain substances, or who want to avoid certain animal products for religious or cultural reasons may need to know about the origin/source of drugs and excipients contained within their medicines. This document provides information to assist clinicians in dealing with these types of situations. Background A number of medicines (including tablets, injections, capsules, creams, mixtures and vaccines) contain animal products or are animal derived. For example, gelatin is a partially hydrolysed collagen which is usually bovine (beef) or porcine (pig) in origin.
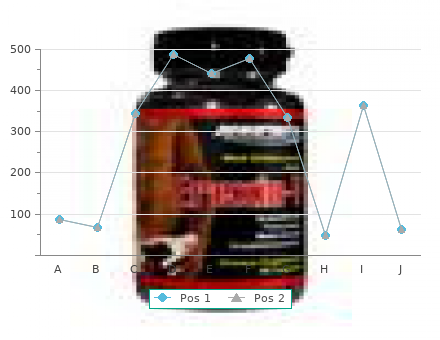
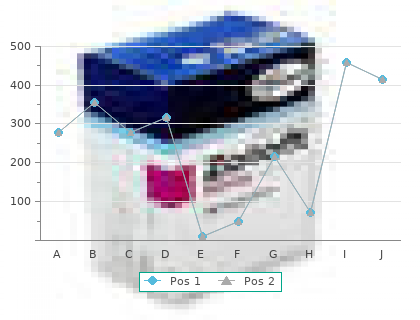
High- incomes in four of the survey countries have higher rates income Americans were as or more likely to report cost- of use than in this the U imitrex 25 mg line muscle relaxant dosage. Percent of Population Reporting Not Filling a Prescription or Skipping a Dose Because of Cost During the Previous 12 Months Unadjusted odds ratio Adjusted odds ratio Country rates (95% confdence interval) (95% confdence interval) United States 23. Prescription Drug Accessibility and Affordability in the United States and Abroad 5 Exhibit 6. Average income Above-average income Percent 50 out-of-Pocket Costs 40 Even with their higher rate of unfulfilled prescriptions, 30 Americans are much more likely than residents of the 20 other countries to report out-of-pocket spending in excess of $1,000 in the previous year. The next highest share of population paying $1,000 or more in out-of-pocket for prescription combined in every country except Australia. This likely reflects gaps in cover- In countries with comprehensive drug benefit age and high cost-sharing that even insured Americans programs that have low copayments—Germany, the often experience. Studies repeatedly find negative national differences in drug prices because standard health and total cost effects from high out-of-pocket pre- doses and package sizes vary from country to country scription costs for patients with chronic disease and other and are seldom taken into account in price comparisons. In other countries, a focus on health secure savings has the effect of driving up the list prices and drug benefit policy designed to provide universal of drugs, there is little doubt that uninsured persons in access to essential treatments works together with group the U. Thus, cross-national dif- Affordability of medicines for individual patients is ferences in drug spending likely result from the combined facilitated by policies that limit cost-sharing for covered effects of higher use of medicines in the U. Most of these countries do so with relatively low cost-sharing by Prescription Drug Accessibility and Affordability in the United States and Abroad 7 patients, especially for vulnerable populations (e. Such comparative assessment review can help spur Canadian system of public drug coverage is comparable both the development and adoption of innovative and to that of the U. However, public programs for coverage under a universal drug benefit system, a finance a greater share of total prescription drug costs in key consideration is the price that can be charged. In Canada, prices are limited in com- to geography, age, income, or employment—can be parison to those charged in seven comparator countries cost-effective when viewed from health system and (including the U. Consider public benefits in and 2) relative pricing policies and negotiations concern- New Zealand, which operate with a national formulary ing the price of medicines. Different formularies may uses a variety of supplier contracts and coverage policies apply to different patients, depending upon their insurer. Zealand, per capita pharmaceutical spending in the Therefore, the National Institute for Health and Clinical U. In other countries, every medicine is appraised to implied by such a thought experiment is on the order 8 The Commonwealth Fund of $80 billion in 2005 alone. Because uninsured management occurs despite the fact that the underlying Americans are currently more likely than their insured health systems are based on social insurance models with counterparts to go without prescribed medications, this 13 many competing insurers. One message from mation to guide and inform benefit designs and pricing abroad is clear: sustainability, affordability, and equity in policies can help moderate cost increases while assuring pharmaceutical coverage will require commitment to uni- access to effective medications, including new products. Interviews were conducted with 1,000 adults in Australia and in New Zealand; 1,500 adults in Germany, in the Netherlands, and in the United Kingdom; 2,500 adults in the United States; and 3,000 adults in Canada. In our analyses, we weighted individual responses to be representative of national populations. Where we report shares of populations providing specific answers to survey questions, we used chi-squared tests to determine whether there were statistically significant differences between countries and to determine whether there were statistically significant differences across age, income, and health status within countries. We report adjusted odds ratios that compare specific results across all countries, using the U. These models are adjusted for sex, age, income, and health status (number of chronic conditions reported). We com- pare accessibility results across specific subpopulations of working-age adults in the U. Prescription Drug Accessibility and Affordability in the United States and Abroad 9 8 Notes R. Copayment on Rational Drug Use,” Cochrane 3 Database of Systematic Reviews: Reviews, Jan. Ross-Degnan, “The Case for a Medicare Policy Systems: A ‘Triple-A’ Framework and Example Drug Coverage Benefit: A Critical Review of the Analysis,” The Open Health Services and Policy Journal, Empirical Evidence,” Annual Review of Public 2009 2(1):1–9; J. Goetzel, “The Effects of States and Canada: A System-Level Comparison Prescription Drug Cost Sharing: A Review of the Using the 2007 International Health Policy Survey Evidence,” American Journal of Managed Care, in Seven Countries,” Clinical Therapeutics, Jan. Berkman, “Social Epidemiology: Social Prescription Drugs: Coverage, Cost-Sharing, and Determinants of Health in the United States: Are We Financial Protection in Six European Countries Losing Ground? Descriptions of health care systems: Australia, Canada, Denmark, England, France, Germany, Italy, 12 S. Mitton, the Netherlands, New Zealand, Norway, Sweden, “Centralising Drug Review to Improve Coverage Switzerland, and the United States (New York: The Decisions: Economic Lessons from (and for) Commonwealth Fund, forthcoming).
Limited epidemiological evidence suggests that exposure to aged bird droppings may increase risk of infection purchase imitrex 25 mg free shipping spasms near kidney. Patients with isolated cryptococcal antigenemia without meningitis can be treated similarly to patients with focal pulmonary cryptococcosis (see below). Treating Disease Treating cryptococcosis consists of three phases: induction, consolidation, and maintenance therapy. Historically, amphotericin B deoxycholate has been the preferred formulation at a dose of 0. However, there is a growing body of evidence that lipid formulations of amphotericin B are effective for disseminated cryptococcosis, particularly in patients who experience clinically significant renal dysfunction during therapy or who are likely to develop it. When using flucytosine, serum levels of flucytosine, if this assay is available, should be obtained 2 hours post-dose after 3 to 5 doses have been administered. The dose of flucytosine should be reduced by 50% for every 50% decline in creatinine clearance. Fluconazole alone, based on early fungicidal activity, is inferior to amphotericin B22 for induction therapy and is recommended only for patients who cannot tolerate or do not respond to standard treatment. Most of the data on use of these extended-spectrum triazole antifungals have been reported for treatment of refractory cases, with success rates of approximately 50%. In contrast to the other African study, this study used deoxycholate amphotericin B (0. All the triazole antifungals have the potential for complex, and possibly bidirectional, interactions with certain antiretroviral agents. Table 5 lists these interactions and recommendations for dosage adjustments, where feasible. Lumbar opening pressure should be measured in all patients with cryptococcal meningitis at the time of diagnosis. Patients treated with amphotericin B formulations should be monitored for dose-dependent nephrotoxicity and electrolyte disturbances. Pre-infusion administration of 500 to 1000 mL of normal saline appears to reduce the risk of nephrotoxicity during amphotericin B treatment. In patients receiving flucytosine, dosage should be adjusted based on changes in creatinine clearance and can be guided by flucytosine levels. Peak serum flucytosine levels should be obtained 2 hours after an oral dose and the therapeutic range is between 25 and 100 mg/L. Patients treated with flucytosine also should be monitored for hepatotoxicity and gastrointestinal toxicities. Isolates collected to evaluate for persistence or relapse should, however, be checked for susceptibility and compared with the original isolate. While clinical data are lacking, strains with minimum inhibitory concentrations against fluconazole ≥16 µg/mL in patients with persistent disease or relapse may be considered resistant. Patients who fail to respond to induction with fluconazole monotherapy should be switched to amphotericin B, with or without flucytosine. Those initially treated with an amphotericin B formulation should remain on it until a clinical response occurs. The newer triazoles—posaconazole and voriconazole—have activity against Cryptococcus spp. Special Considerations During Pregnancy The diagnosis of cryptococcal infections during pregnancy is similar to that in non-pregnant adults. Lipid formulations of amphotericin B are the preferred initial regimen for the treatment of cryptococcal meningoencephalitis, disseminated disease, or severe pulmonary cryptococcosis in pregnant patients. Extensive clinical experience with amphotericin has not documented teratogenicity. Neonates born to women on chronic amphotericin B at delivery should be evaluated for renal dysfunction and hypokalemia. Flucytosine was teratogenic in animal studies, and human experience is limited to case reports and small series. Congenital malformations similar to those observed in animals, including craniofacial and limb abnormalities, have been reported in infants born to mothers who received fluconazole at doses of ≥400 mg/ day or more through or beyond the first trimester of pregnancy. Use of fluconazole in the first trimester should be considered only if the benefits clearly outweigh risks.